How Hormones Affect Weight: A Complete Guide for Women
RHC · Pre/Postnatal Fitness Specialist
The relationship between hormones and weight is real, complex, and often misunderstood. Hormonal factors don't override the fundamentals of energy balance, but they significantly influence appetite, fat storage patterns, where the body stores fat, and how efficiently metabolism works.
For women especially, navigating the hormonal landscape, across the menstrual cycle, reproductive years, perimenopause, and beyond, is central to understanding body weight.

The Key Hormones and Their Weight Effects
Oestrogen
Oestrogen is the primary female sex hormone, produced mainly by the ovaries during reproductive years. Its effects on body composition are significant:
Fat distribution: Oestrogen promotes fat storage at the hips, thighs, and buttocks, the typical premenopausal female pattern. This subcutaneous fat is relatively metabolically inert. When oestrogen declines (perimenopause, post-pill withdrawal, hypothalamic amenorrhea), fat redistributes to the abdomen.
Insulin sensitivity: Oestrogen improves insulin sensitivity, making carbohydrate metabolism more efficient. Declining oestrogen reduces insulin sensitivity, the same carbohydrate intake that was previously well-tolerated begins causing higher blood glucose and increased fat storage.
Muscle maintenance: Oestrogen supports muscle protein synthesis. Its decline accelerates muscle loss and reduces resting metabolic rate.
Influence over the menstrual cycle: Oestrogen peaks in the follicular phase (days 1-14), this phase is associated with better energy, improved insulin sensitivity, and somewhat easier fat loss. The luteal phase (days 15-28), dominated by progesterone with declining oestrogen, brings increased appetite, water retention, and slightly reduced insulin sensitivity.
Progesterone
Progesterone rises in the luteal phase after ovulation. Its weight-related effects:
- Increases appetite: Specifically cravings for carbohydrates and sweet foods
- Causes water retention: Can add 0.5-2.5kg to scale weight in the luteal phase
- Competes with aldosterone: Has mild diuretic properties, when progesterone drops at menstruation, this effect disappears and the water retention may briefly worsen
These effects explain why the week before menstruation feels bloated and hungry regardless of dietary habits.
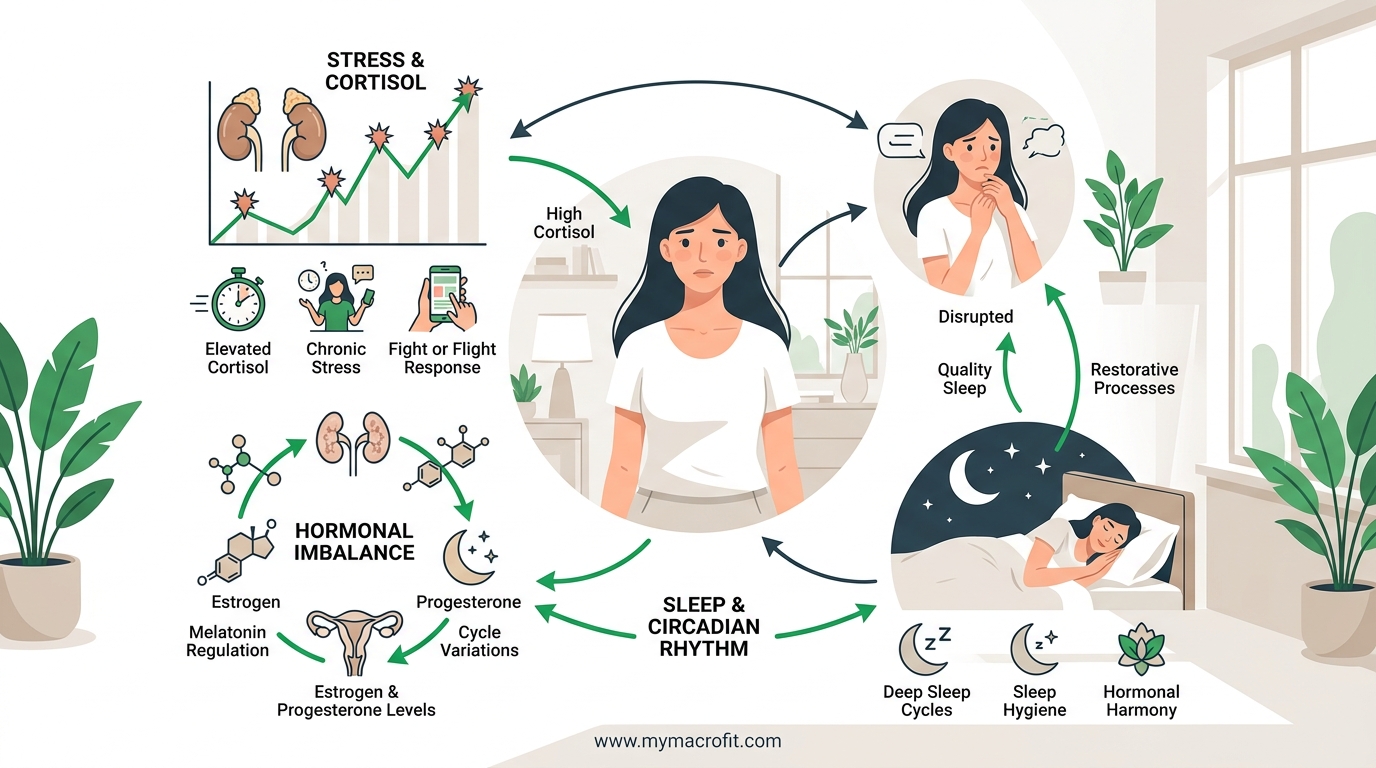
Cortisol
See our cortisol and weight gain guide for the full mechanism. In summary: chronically elevated cortisol promotes visceral fat storage, increases ghrelin, reduces leptin, breaks down muscle, and causes water retention.
Women are particularly susceptible to cortisol-driven abdominal fat post-menopause when oestrogen's buffering effect on cortisol is reduced.
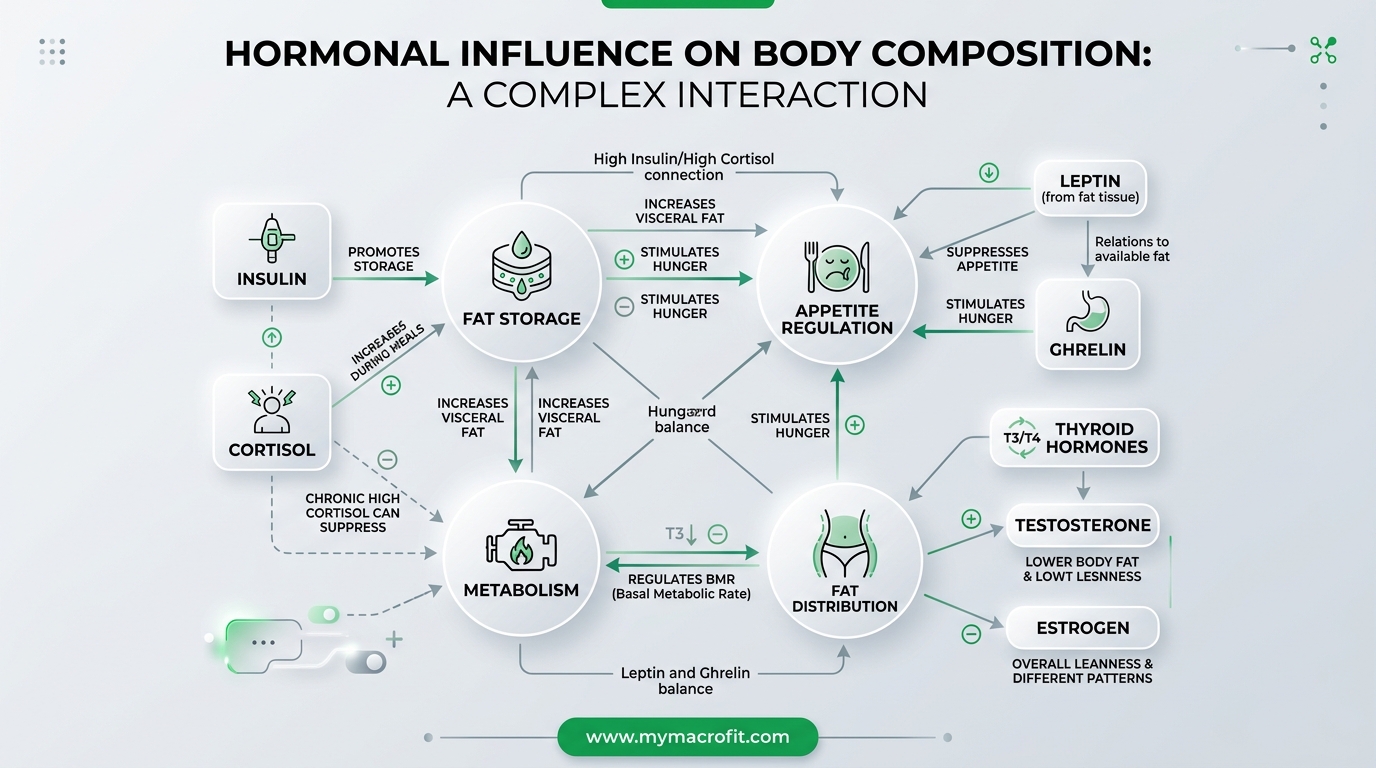
Insulin
Insulin is the primary fat-storage hormone. When blood glucose rises, insulin is released to direct glucose into cells. Chronically high insulin (insulin resistance) keeps fat locked in storage.
Insulin resistance in women is associated with:
- PCOS (polycystic ovary syndrome), affects 10-15% of women of reproductive age
- Perimenopause and menopause
- Poor diet (high in refined carbohydrates and processed foods)
- Sedentary lifestyle
- Excess visceral fat (which itself promotes insulin resistance, a vicious cycle)
Improving insulin sensitivity: Resistance training is the most potent lifestyle intervention, it upregulates GLUT-4 transporters in muscle, improving glucose uptake independently of insulin. A lower-glycaemic diet and adequate sleep also improve insulin sensitivity significantly.
Leptin and Leptin Resistance
Leptin is the satiety hormone produced by fat cells. It signals to the brain that energy stores are adequate and suppresses appetite. In principle, the more fat stored, the more leptin produced, the less hungry you are.
In practice, many overweight individuals develop leptin resistance, the brain stops responding to leptin's signals despite high circulating levels. The result is persistent hunger despite adequate or excess energy stores.
What impairs leptin sensitivity:
- Chronic overconsumption of high-fat, high-sugar foods
- Poor sleep (one of the most significant causes)
- Chronic inflammation
- High triglycerides (physically block leptin transport to the brain)
Improving leptin sensitivity: Reducing ultra-processed food, improving sleep quality, reducing triglycerides through dietary fat quality improvement, and regular exercise all improve leptin signalling.
Ghrelin
Ghrelin is the hunger hormone produced primarily in the stomach. It rises before meals and drops after eating. It spikes significantly with sleep deprivation and calorie restriction.
Women and ghrelin: Research suggests women may have higher ghrelin responses to certain triggers (including psychological stress) than men. This partly explains why stress eating is more prevalent in women.
Reducing ghrelin: Adequate sleep (ghrelin rises significantly with sleep under 6 hours), adequate protein at meals (protein suppresses ghrelin more effectively than carbs or fat), and avoiding excessive calorie restriction.
Thyroid Hormones (T3 and T4)
The thyroid regulates basal metabolic rate. Hypothyroidism (underactive thyroid), significantly more common in women than men, reduces metabolic rate and can cause weight gain, fatigue, cold sensitivity, constipation, and hair thinning.
Hashimoto's thyroiditis (autoimmune hypothyroidism) is the most common cause in women, often developing in the 30s-50s.
If you suspect hypothyroidism: Request a thyroid function test from your GP. TSH, free T4, and TPO antibodies (for Hashimoto's) are the relevant markers. Treated hypothyroidism with appropriate levothyroxine dose typically resolves the metabolic rate reduction.
The Menstrual Cycle and Weight Fluctuation
Understanding normal hormonal weight variation across the cycle prevents unnecessary panic:
Days 1-5 (menstruation): Scale weight often drops as water retention from the luteal phase releases. Energy may be lower; iron loss occurs.
Days 6-14 (follicular phase): Oestrogen rising, best energy, best insulin sensitivity, scale weight typically at monthly low. Easiest phase for fat loss.
Day 14 (ovulation): Brief temperature rise, possible 0.5kg fluid gain.
Days 15-28 (luteal phase): Progesterone dominant, appetite increases, particularly for carbohydrates. Water retention builds gradually. Scale may be 1-3kg higher than follicular phase. Training capacity may be slightly reduced.
This pattern means scale weight can fluctuate 1-3kg across a month entirely from hormonal fluid changes, with no change in fat. This is normal physiology.
Supporting Hormone Balance Through Nutrition
For insulin sensitivity: Prioritise fibre-rich whole foods, reduce refined carbohydrates, include resistance training, maintain adequate magnesium and zinc.
For cortisol: Prioritise sleep (the single most effective intervention), moderate caffeine, manage stress, avoid very large calorie deficits.
For thyroid function: Ensure adequate iodine (seafood, dairy, iodised salt), selenium (brazil nuts, tuna), and zinc. Avoid excessive raw cruciferous vegetables if thyroid issues are suspected (cooking deactivates goitrogens).
For leptin sensitivity: Improve sleep quality, reduce ultra-processed food, maintain omega-3 intake to reduce inflammation, include adequate dietary fat.
The Bottom Line
Hormones are not an excuse, they're a real biological context. Understanding which hormones are influencing your weight, at what life stage, and through what mechanisms allows you to target your interventions more precisely.
For most women, the combination of adequate protein, resistance training, quality sleep, and stress management addresses the most significant hormonal barriers to weight management simultaneously.
Where specific hormonal conditions are suspected (hypothyroidism, PCOS, insulin resistance), medical diagnosis is the appropriate next step.
Save & share on Pinterest
Click any card to pin it — or share with someone who needs it.
How Hormones Affect Weight: A Complete Guide for Women
The key hormones that influence female body weight, oestrogen, progesterone, cortisol, insulin, lept…
The key hormones that influence female body weight, oestrogen, progesterone, cor…
Read the full guide: How Hormones Affect Weight: A Complete Guide for Women
Free fitness tools
How Hormones Affect Weight: A Complete Guide for Women — use our free calculators for instant person…
Pinterest opens in a new tab. You can edit the description before saving.
Frequently Asked Questions
Which hormones cause weight gain in women?+
Can hormonal imbalance prevent weight loss?+
How do I know if my weight issues are hormonal?+
Can I balance my hormones naturally to lose weight?+
Do I need hormone testing before trying to lose weight?+
About the Author

I'm a registered health coach and pre/postnatal specialist. I look at the whole person, your sleep, your stress, your hormones, because the number on the scale is only ever part of the story.
View full profile →