
Inositol vs Metformin vs GLP-1: Which Is Best for PCOS and Insulin Resistance?
RHC · Pre/Postnatal Fitness Specialist
If you have PCOS or insulin resistance and you've been researching weight loss, you've run into the same three names again and again: inositol, metformin, and the GLP-1 medications like Ozempic and Mounjaro. They all target the insulin resistance that drives so much PCOS weight gain, but they're very different tools, with very different trade-offs. Here's an honest comparison to take into a conversation with your doctor.
Important: this is educational information, not medical advice. Metformin and GLP-1s are prescription medications, and even supplements interact with your individual health. Every decision here belongs with a qualified clinician who knows your history.
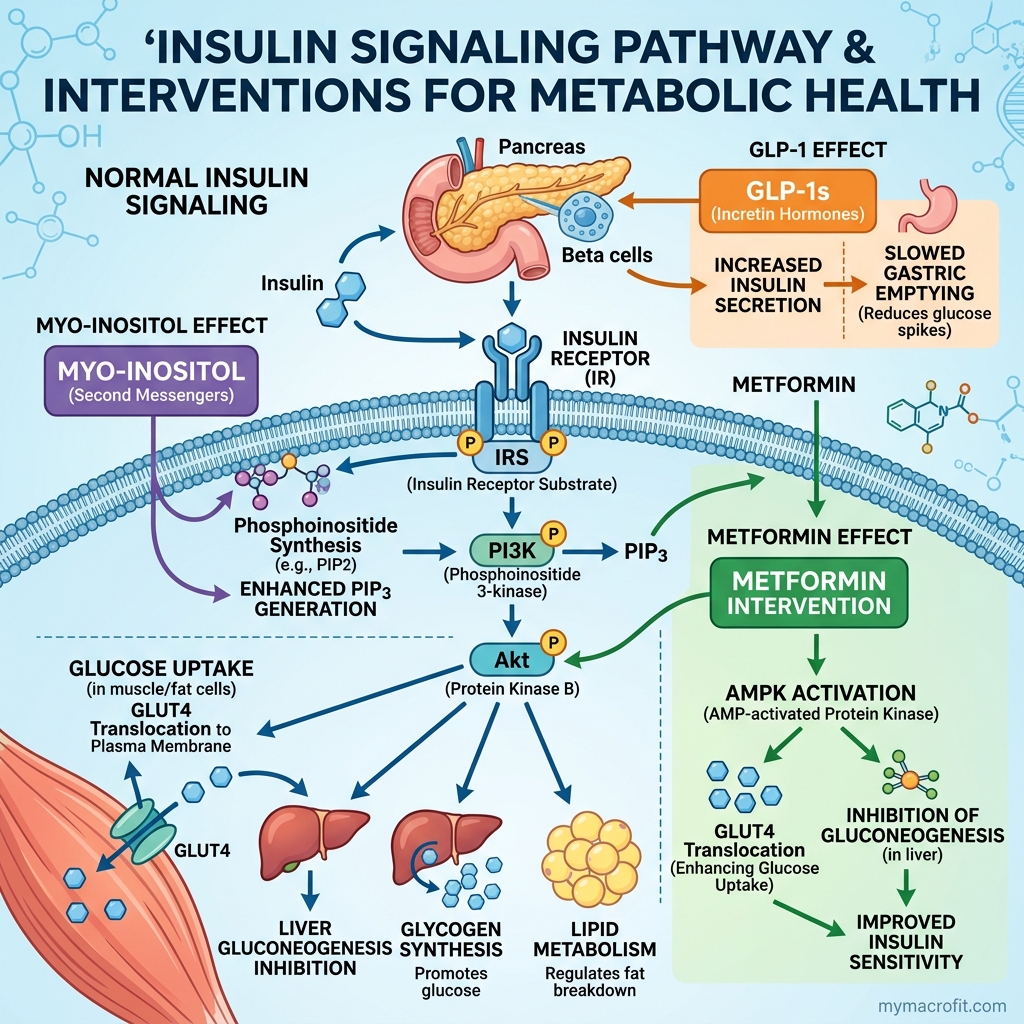
Why insulin resistance is the common target
First, the thing all three have in common. In many women with PCOS, the underlying engine of weight gain, irregular cycles, and raised androgens is insulin resistance, the body's cells respond poorly to insulin, so it produces more, and high insulin promotes fat storage and disrupts ovarian hormones.
Improve insulin sensitivity and the whole picture tends to ease: weight becomes more manageable, cycles can regulate, and symptoms like acne and excess hair can improve. Inositol, metformin, and GLP-1s each chip away at this problem from a different angle.
Inositol: the gentle first-line option
Inositol is a naturally occurring compound (technically a sugar alcohol) that helps cells respond to insulin. The most-studied form for PCOS is myo-inositol, often paired with a small amount of D-chiro-inositol in a 40:1 ratio that mirrors the body's natural balance.
- What it does well: head-to-head trials show it can match metformin for improving insulin sensitivity and ovulation in many women, with far fewer side effects, especially the digestive upset metformin is known for.
- The trade-offs: it's gentler, so effects are gradual (give it ~3 months), and it's not a fit for every case. It's a supplement, not a drug, which means lighter oversight but also less regulation of product quality.
- Typical protocol: 4g myo-inositol daily, usually with 400mcg folic acid.
For many women, inositol is a sensible, low-risk first thing to try. We cover it in depth in our dedicated inositol for PCOS guide.
Metformin: the established prescription
Metformin is a decades-old prescription medication for type 2 diabetes that's widely used off-label for PCOS. It lowers the amount of glucose your liver releases and improves insulin sensitivity.
- What it does well: a long, well-understood track record, cheap, and genuinely effective at improving insulin markers and supporting modest weight management in PCOS.
- The trade-offs: digestive side effects (nausea, diarrhoea) are common, especially at first, and are the main reason people stop. It requires a prescription and monitoring.
- Where it fits: a proven option when inositol isn't enough, or as a first-line choice your doctor prefers, and sometimes used alongside inositol, since they work through somewhat different pathways.
GLP-1 medications: the powerful, intensive tool
GLP-1 receptor agonists (semaglutide/Ozempic, tirzepatide/Mounjaro) are a different category entirely. Rather than gently improving insulin sensitivity, they powerfully reduce appetite, producing far larger average weight loss than either inositol or metformin.
- What it does well: the biggest weight-loss effect by a wide margin, plus genuine improvements in insulin resistance as weight comes down.
- The trade-offs: prescription-only, expensive, real side effects (nausea, gallbladder issues, muscle-loss risk), and weight tends to return when the medication stops. They're an intensive intervention, not a casual one.
- Where it fits: typically considered for higher BMI or when first-line approaches haven't delivered, a decision firmly in medical hands. We cover the natural side of this in GLP-1 vs natural weight loss.
How to think about choosing
A rough way to frame the conversation with your doctor:
- Start gentle, escalate as needed. Many clinicians and women begin with lifestyle plus inositol, move to metformin (or add it) if that's insufficient, and reserve GLP-1s for cases that need a stronger tool.
- Side-effect tolerance matters. Inositol is the easiest on the body; metformin's digestive effects put some people off; GLP-1s carry the most significant side-effect profile.
- None of them replaces the basics. A lower-GI, higher-protein diet, resistance training, and good sleep remain the foundation under every option, the medications and supplements work with those habits, not instead of them.

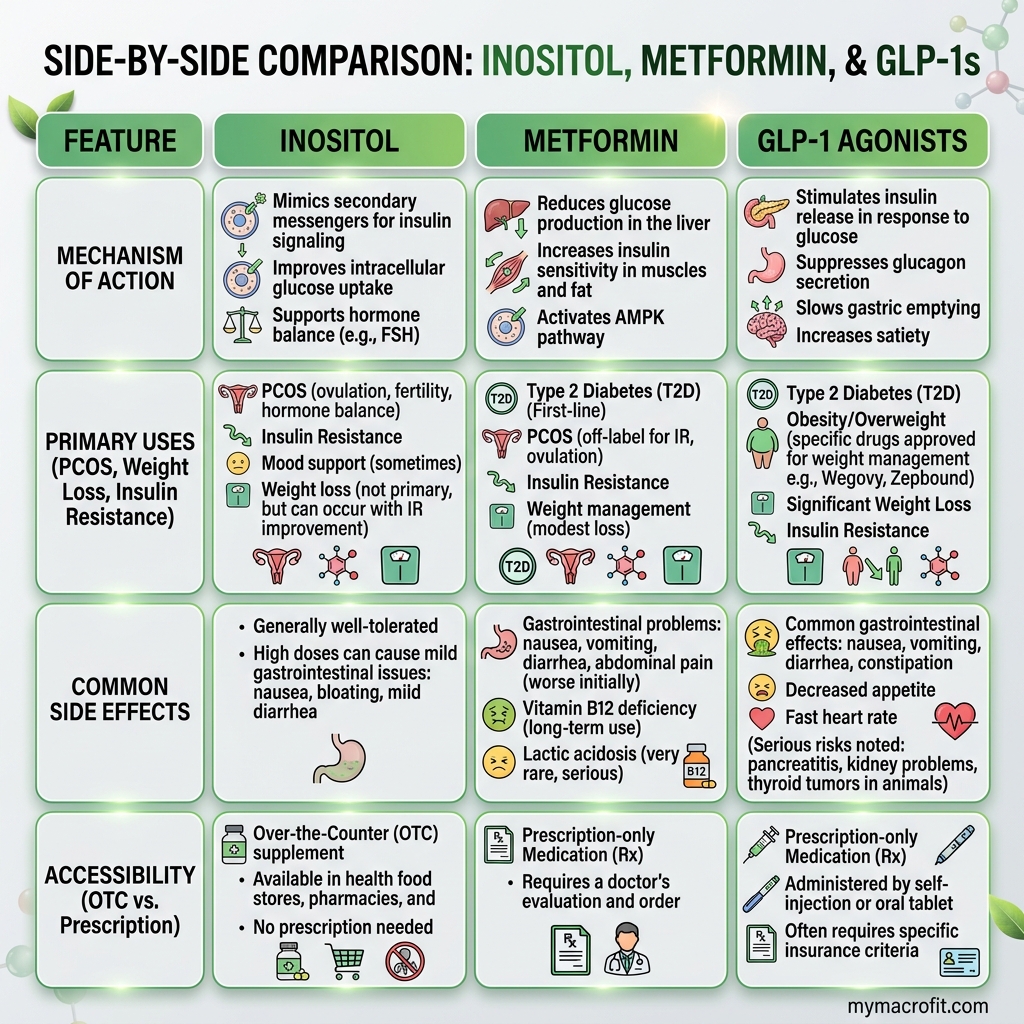
The three at a glance
To bring the comparison together, here's how the options line up on the factors that usually matter most in a conversation with your doctor. Treat this as a discussion starter, not a recommendation:
| Inositol | Metformin | GLP-1 | |
|---|---|---|---|
| Type | Supplement | Prescription drug | Prescription drug |
| Main action | Improves insulin sensitivity | Improves insulin sensitivity | Reduces appetite |
| Avg weight effect | Modest | Modest | Large |
| Side effects | Minimal (mild GI) | GI common early | Nausea, GI, others |
| Cost | Low | Low | High |
| Typical place | Gentle first-line | Established first-line | Intensive, later-line |
| Time to assess | ~3 months | A few weeks | Weeks |
Read across and you can see they're not really competitors so much as rungs on a ladder, from gentlest to most intensive. Most women and clinicians start low and escalate only if needed, which is why "which is best" almost always answers to "best for you, right now, in your doctor's judgement."
Build on the same foundation either way
Whichever rung you and your doctor land on, notice the row that doesn't appear in the table because it underpins all three: your daily habits. A lower-GI, protein-forward way of eating, regular strength training, and protecting your sleep improve insulin sensitivity on their own, and they make every one of these tools work better. Many women find that lifestyle plus inositol is enough; others need more support, and that's not a failure, it's just biology. The kindest thing you can do is treat the medication or supplement as a helper sitting on top of habits that nourish you, rather than a replacement for them.
The bottom line
There's no single winner here, there's the right fit for your body, your symptoms, your side-effect tolerance, and your doctor's judgement. Inositol is a strong, low-risk first option with surprisingly good evidence. Metformin is the established prescription workhorse. GLP-1s are the powerful but intensive tool for when more is needed. Bring this comparison to your healthcare provider and decide together, and whatever you choose, build it on the dietary and training foundation that makes all three work better.
Save & share on Pinterest
Click any card to pin it — or share with someone who needs it.
Inositol vs Metformin vs GLP-1: Which Is Best for PCOS and Insulin Resistance?
Inositol, metformin, and GLP-1 medications all target the insulin resistance behind PCOS weight gain…
Inositol, metformin, and GLP-1 medications all target the insulin resistance beh…
Read the full guide: Inositol vs Metformin vs GLP-1: Which Is Best for PCOS and Insulin Resistance?
Free fitness tools
Inositol vs Metformin vs GLP-1: Which Is Best for PCOS and Insulin Resistance? — use our free calcul…
Pinterest opens in a new tab. You can edit the description before saving.
Frequently Asked Questions
Is inositol as effective as metformin for PCOS?+
Can you take inositol and metformin together?+
How does inositol compare to GLP-1 medications like Ozempic for PCOS?+
What is the right inositol dosage for PCOS?+
Do you have to take medication for PCOS weight loss, or can diet work?+
How long should I try one option before considering another?+
Are there risks to taking inositol if I don't actually have insulin resistance?+
About the Author

I'm a registered health coach and pre/postnatal specialist. I look at the whole person, your sleep, your stress, your hormones, because the number on the scale is only ever part of the story.
View full profile →

