The Complete Hormone Balance Guide for Women
RHC · Pre/Postnatal Fitness Specialist
Hormones are the body's chemical messaging system, nanogram quantities circulating in the blood that regulate metabolism, body composition, energy, reproduction, mood, and sleep. When they're balanced, everything works. When they're not, seemingly every system suffers simultaneously.
For women specifically, hormonal health is complex: the monthly cycling of oestrogen and progesterone interacts with thyroid hormones, insulin, cortisol, and androgens in ways that profoundly affect how you look, feel, and respond to diet and exercise.
This guide explains the key hormones, how they interact, what disrupts them, and, most importantly, what evidence-based interventions actually restore balance.

The Key Hormones and Their Roles
Oestrogen (Oestradiol, E2)
Oestrogen is the primary female sex hormone, produced mainly by the ovaries (and in smaller amounts by adipose tissue and the adrenal glands). Beyond reproduction, oestrogen:
- Protects against visceral fat accumulation (fat is redistributed to abdomen when oestrogen declines)
- Supports insulin sensitivity
- Supports bone density
- Regulates serotonin and dopamine production
- Supports muscle protein synthesis
- Maintains cardiovascular health
What disrupts oestrogen balance:
- Perimenopause and menopause (physiological decline)
- Excess body fat (adipose tissue converts androgens to oestrogen, can cause relative oestrogen excess)
- Endocrine-disrupting chemicals (plastics, pesticides)
- Disrupted gut microbiome (impairs oestrogen recirculation via the estrobolome)
- Excessive alcohol
Progesterone
Progesterone is produced primarily by the corpus luteum after ovulation. It counterbalances oestrogen's proliferative effects and plays a critical role in the second half of the menstrual cycle.
Low progesterone effects:
- Irregular or absent periods
- Sleep disturbance (progesterone is mildly sedative)
- Anxiety and mood disruption
- Relative oestrogen dominance symptoms (heavy periods, bloating, breast tenderness)
What depletes progesterone:
- Anovulatory cycles (no ovulation = no corpus luteum = no progesterone)
- Chronic stress (cortisol steals progesterone via the "pregnenolone steal")
- Under-fuelling (undereating suppresses the hypothalamic-pituitary-ovarian axis)
Insulin
Insulin is produced by the pancreas and regulates blood glucose. While not a sex hormone, insulin is one of the most metabolically influential hormones in the body and profoundly affects hormonal health:
- Excess insulin drives androgen production in the ovaries (key mechanism in PCOS)
- Insulin resistance impairs glucose disposal, driving higher insulin secretion
- Chronic high insulin promotes fat storage, particularly visceral fat
- Insulin interacts with leptin and ghrelin to regulate appetite
Improving insulin sensitivity is often the linchpin of hormonal rebalancing, particularly for women with PCOS, insulin resistance, or weight-related hormonal disruption.
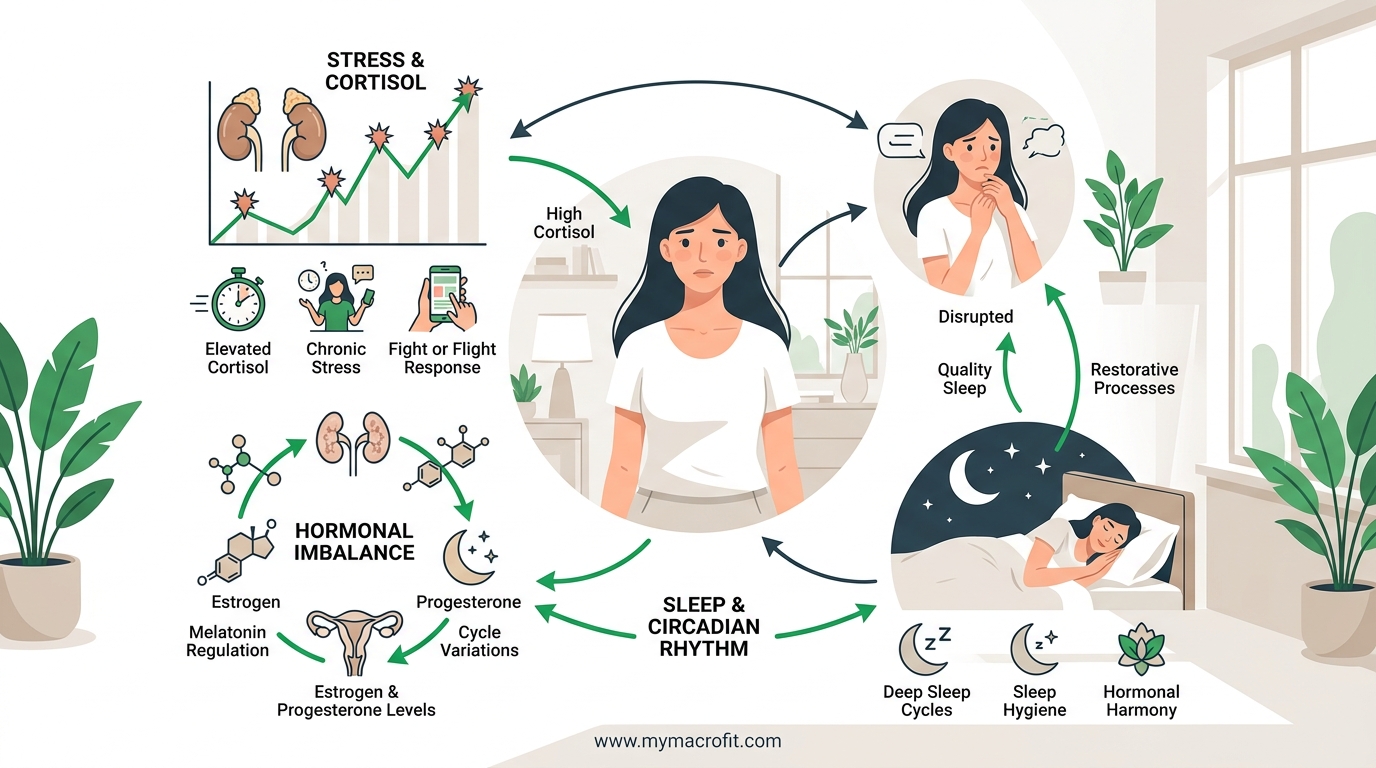
Cortisol
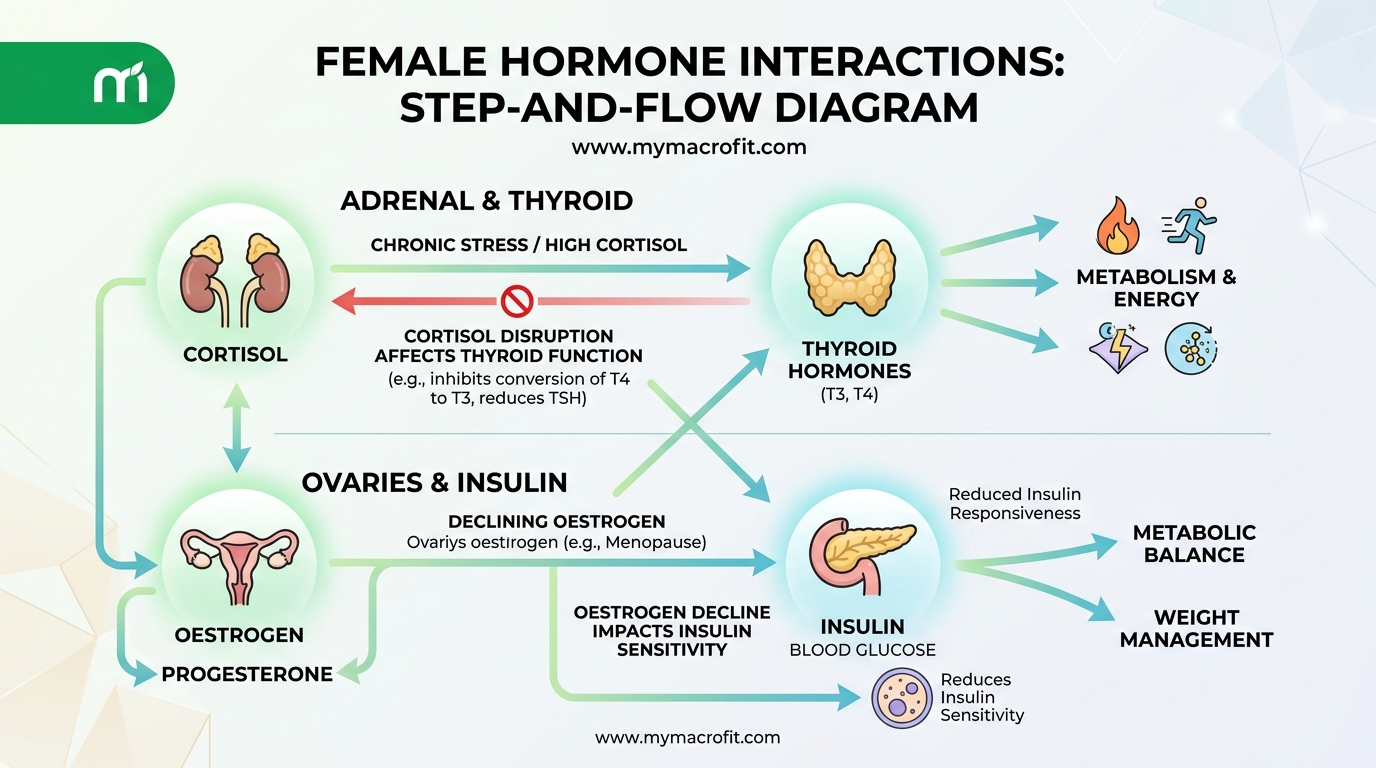
Cortisol is the primary glucocorticoid produced by the adrenal glands in response to stress (physical or psychological). Short-term cortisol elevation is adaptive. Chronic elevation is destructive:
- Suppresses GnRH → reduces LH/FSH → disrupts ovulation
- Promotes abdominal fat storage
- Drives insulin resistance
- Reduces thyroid hormone conversion (T4 to active T3)
- Depletes progesterone via the pregnenolone steal
- Disrupts sleep (cortisol is the waking hormone, it should be lowest at night)
For a detailed look at cortisol and weight, see our cortisol and weight gain guide.
Thyroid Hormones (T3, T4, TSH)
The thyroid regulates metabolic rate. Hypothyroidism (underactive thyroid) is more common in women than men and increases with age. Even subclinical hypothyroidism (elevated TSH with normal T3/T4) is associated with:
- Unexplained weight gain and difficulty losing weight
- Fatigue
- Cold sensitivity
- Hair loss and brittle nails
- Brain fog
- Constipation
Dietary factors relevant to thyroid: adequate iodine (deficiency impairs T4 production), selenium (required for T4→T3 conversion), zinc, and iron. See our Hashimoto's and weight loss guide for autoimmune thyroid context.
Testosterone
Often overlooked in women's health, testosterone is produced in small amounts by the ovaries and adrenal glands and plays an important role in:
- Libido and sexual response
- Muscle building and strength
- Bone density
- Motivation and energy
- Cognitive function
Both deficiency (hypoactive sexual desire, fatigue, muscle loss) and excess (androgenisation in PCOS, acne, hirsutism, scalp hair thinning) are clinically relevant in women.
Common Hormonal Conditions
Polycystic Ovary Syndrome (PCOS)
PCOS affects approximately 10% of reproductive-age women and is the most common endocrine disorder in this group. It is characterised by:
- Irregular or absent ovulation
- Elevated androgens (testosterone)
- Multiple small ovarian cysts (not required for diagnosis)
- Often (but not always) insulin resistance
The insulin-PCOS connection: In insulin-resistant PCOS, excess insulin stimulates the ovaries to produce testosterone. This is why dietary interventions targeting insulin sensitivity are among the most effective PCOS management strategies.
For a detailed PCOS intervention protocol, see our PCOS 8-week plan.
Hypothalamic Amenorrhoea (HA)
HA is the suppression of the hypothalamic-pituitary-ovarian axis due to inadequate energy availability. The body interprets under-fuelling as a famine and suppresses reproduction as a survival mechanism.
Signs: Loss of periods in a young woman with no other hormonal explanation. Often occurs in women who are training heavily, restricting calories significantly, or are at low body weight.
Treatment: Increased calorie intake and reduced training volume. Recovery of periods typically takes 3-6 months of consistent adequate fuelling.
Perimenopause and Menopause
The transition from reproductive to post-reproductive hormonal status, characterised by declining and erratic oestrogen and progesterone. For a comprehensive guide, see our Perimenopause & Menopause Guide.
Nutrition for Hormonal Balance
1. Calorie Adequacy, The Non-Negotiable Foundation
Under-eating is one of the most common causes of hormonal disruption in active women. The hypothalamus monitors energy availability, when it detects inadequate fuel relative to energy expenditure, it suppresses the reproductive and thyroid axes.
Signs of under-fuelling: Loss of periods, persistent fatigue, cold hands/feet, persistent low mood despite adequate sleep, hair shedding, and poor recovery from training.
Minimum: Most active women need at least 1,600-1,800 kcal/day to maintain hormonal function. Women training 4+ days/week likely need 2,000+ kcal. Use our TDEE Calculator as a starting point.
2. Carbohydrates and Insulin Sensitivity
Carbohydrate quality and distribution significantly affects insulin levels, which cascade to affect androgen production, appetite regulation, and oestrogen balance.
For insulin-resistant PCOS:
- Prioritise low-glycaemic carbohydrates (legumes, oats, sweet potato, quinoa)
- Distribute carbohydrates across 3 main meals rather than concentrating them
- Combine carbohydrates with protein and fat to slow glucose absorption
- Consider lower total carbohydrate intake (100-120g/day) as a starting point for significant insulin resistance
For general hormonal balance: Carbohydrates are not the enemy, severely low carbohydrate diets can suppress thyroid function and increase cortisol in women. A moderate approach with emphasis on food quality outperforms extreme restriction.
3. Fat, Essential for Hormone Production
Every steroid hormone (oestrogen, progesterone, testosterone, cortisol) is synthesised from cholesterol. Dietary fat, particularly saturated and monounsaturated fat, is essential for hormone production.
Very low-fat diets (under 20% calories from fat) are consistently associated with lower testosterone and oestrogen levels. Women need adequate dietary fat to maintain hormonal health.
Key fats:
- Olive oil (oleic acid, anti-inflammatory, supports oestrogen metabolism)
- Oily fish (omega-3 EPA/DHA, reduces prostaglandins that drive period pain, reduces systemic inflammation)
- Eggs and full-fat dairy (cholesterol and saturated fat, hormone precursors)
- Avocado and nuts (monounsaturated fat, vitamin E)
Minimum fat intake: 0.8-1g per kg bodyweight (approximately 60-80g for a 70kg woman). Do not drop below this consistently.
4. Supporting Oestrogen Metabolism
The gut microbiome plays a direct role in oestrogen recycling through the "estrobolome", a collection of gut bacteria that metabolise oestrogens. Poor gut health can impair this process, contributing to oestrogen excess or deficiency.
Supporting oestrogen metabolism:
- High-fibre diet (30g/day) to support beneficial bacteria
- Cruciferous vegetables (broccoli, cauliflower, Brussels sprouts), contain indole-3-carbinol and DIM, which support oestrogen hydroxylation to less potent forms
- Ground flaxseed, lignans support oestrogen metabolism
- Fermented foods for microbiome diversity
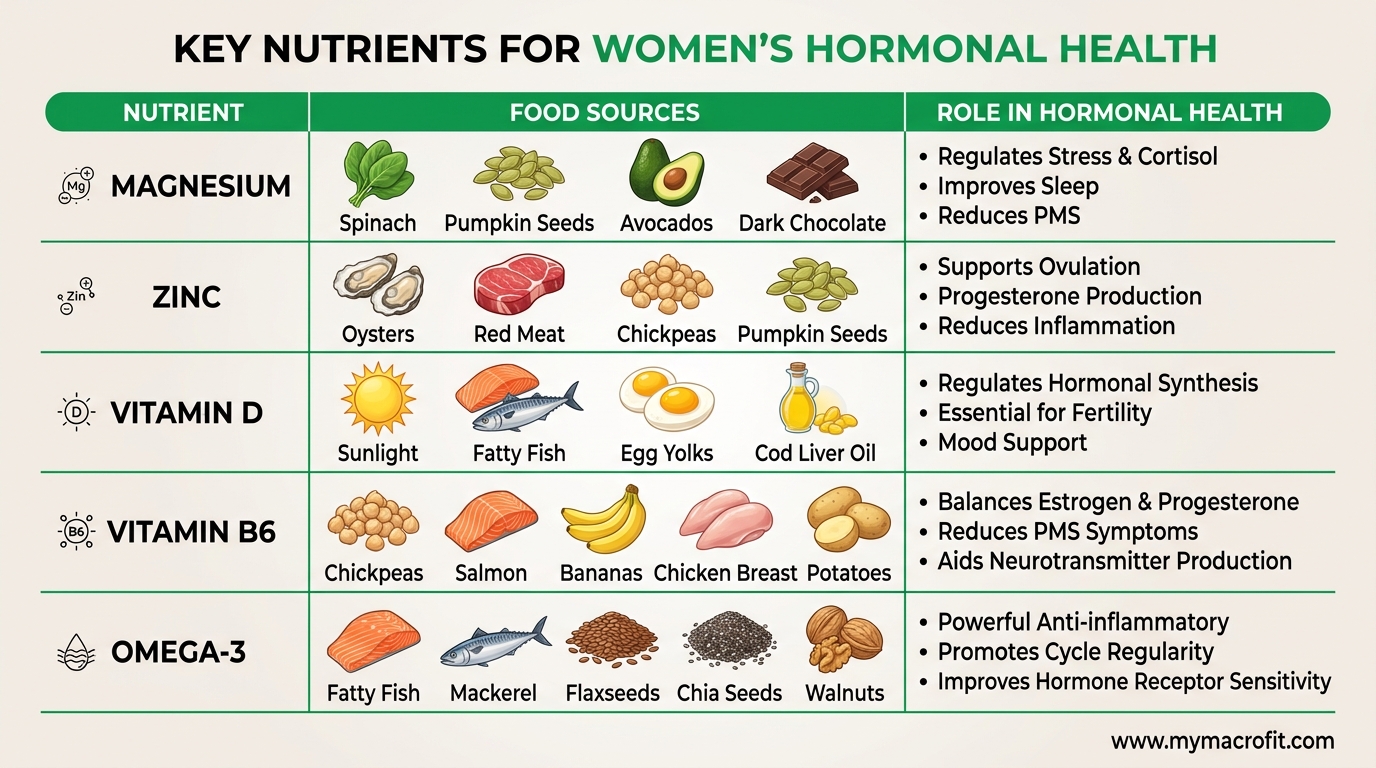
5. Key Micronutrients
Magnesium: Required for 300+ enzymatic reactions. Directly involved in cortisol regulation, insulin signalling, and progesterone balance. Deficiency is common. 300-400mg glycinate form before bed.
Zinc: Required for ovulation, testosterone balance, and thyroid hormone conversion. Found in meat, shellfish, pumpkin seeds. Vegetarians are at higher deficiency risk.
Vitamin D: Functions as a hormone itself. Deficiency is associated with PCOS severity, thyroid dysfunction, and overall metabolic health. 2,000 IU D3 daily (higher if deficient).
B vitamins (particularly B6): B6 directly supports progesterone production and is depleted by oral contraceptives. Found in meat, fish, potatoes, and whole grains.
Iodine and selenium: Essential for thyroid hormone production and conversion. Iodine: seaweed, dairy, iodised salt. Selenium: Brazil nuts (2 per day), fish, meat.
Training for Hormonal Balance
Exercise is hormonal medicine, but the wrong type, wrong volume, or wrong intensity can worsen hormonal balance rather than improve it.
Strength Training
Resistance training is the single most beneficial exercise modality for hormonal health:
- Improves insulin sensitivity (both acutely and chronically)
- Supports testosterone balance
- Reduces cortisol in the long-term (though it acutely raises it)
- Supports oestrogen metabolism through adipose tissue reduction
Target: 3-4 sessions/week of compound strength training.
Cardio: Moderate, Not Excessive
Moderate cardio (zone 2, conversational pace) improves insulin sensitivity, reduces cortisol, and supports cardiovascular health. See our zone 2 training guide.
What to avoid: Excessive high-intensity cardio (6+ sessions/week of HIIT, very high-volume running) without adequate calorie intake. This combination is one of the fastest routes to hypothalamic amenorrhoea and cortisol dysregulation.
Rest and Recovery
Rest days are not optional extras, they're where hormonal recovery occurs. Under-recovered training is a sustained cortisol stimulus that accumulates hormonal disruption over time.
Key Supplements for Hormonal Health
Evidence-supported:
- Magnesium glycinate: 300-400mg/day, cortisol regulation, sleep, insulin sensitivity
- Vitamin D3 + K2: 2,000 IU D3 + 100mcg K2, thyroid function, PCOS, immune health
- Omega-3 (EPA/DHA): 2-3g/day, reduces prostaglandins, supports oestrogen metabolism, anti-inflammatory
Targeted support:
- Inositol (PCOS): 2-4g myo-inositol, insulin sensitising, supports ovulation. See our inositol guide
- Ashwagandha: 300-600mg KSM-66, cortisol reduction, thyroid support. See our ashwagandha guide
- Zinc: 15-25mg/day (with copper if supplementing long-term), ovulation support, androgen balance
When to See a Doctor
Lifestyle interventions are powerful, but they have limits. Seek medical assessment if:
- Periods absent for 3+ months (and not pregnant)
- Significant unexplained weight gain despite calorie deficit
- Symptoms of thyroid dysfunction (severe fatigue, cold intolerance, hair loss, constipation)
- Signs of androgen excess (significant acne, hirsutism, scalp hair loss)
- Planning pregnancy with irregular cycles
- Symptoms that significantly impair daily functioning
A baseline hormonal panel should include: TSH, free T3, free T4, FSH, LH, oestradiol, progesterone (day 21), total and free testosterone, fasting insulin and glucose, DHEA-S, and vitamin D. This gives a comprehensive picture to guide targeted intervention.
The Bottom Line
Hormonal balance in women is the product of four primary inputs: adequate calorie intake, nutritional quality (protein, fat, micronutrients), manageable stress load, and appropriate training. Most hormonal disruption in healthy women without structural disease is responsive to these lifestyle levers, consistently applied over 3-6 months.
Start with the fundamentals: calculate your TDEE and confirm you're eating enough, prioritise protein and dietary fat, add resistance training 3x/week, optimise sleep, and consider targeted supplementation based on your specific symptom pattern.
For a comprehensive downloadable protocol covering all major hormonal conditions, see our Perimenopause Nutrition Guide.
Sources
- Female hormones and body composition: mechanisms, Clegg, Physiology, 2012
- Insulin resistance in PCOS, Diamanti-Kandarakis & Dunaif, Endocrine Reviews, 2012
- Hypothalamic amenorrhoea: causes and treatment, Gordon, Endocrinology and Metabolism Clinics, 2010
- Magnesium and cortisol regulation, Wienecke & Nolden, MMW, 2016
Save & share on Pinterest
Click any card to pin it — or share with someone who needs it.
The Complete Hormone Balance Guide for Women
A science-based guide to female hormones, how they affect weight, energy, mood, and metabolism, and …
A science-based guide to female hormones, how they affect weight, energy, mood, …
Read the full guide: The Complete Hormone Balance Guide for Women
Try the free TDEE Calculator
The Complete Hormone Balance Guide for Women — use our free calculators for instant personalised res…
Pinterest opens in a new tab. You can edit the description before saving.
Ready to get your numbers?
Free calculator, instant results, no signup required.
Frequently Asked Questions
What are the signs of hormonal imbalance in women?+
Can diet fix hormonal imbalance?+
Does stress cause hormonal imbalance?+
How long does it take to rebalance hormones naturally?+
About the Author

I'm a registered health coach and pre/postnatal specialist. I look at the whole person, your sleep, your stress, your hormones, because the number on the scale is only ever part of the story.
View full profile →