
The Complete Women's Fitness Guide: Nutrition, Training, and Hormones
BSc Kinesiology · CPT
I've spent my whole career coaching women, and I've lost count of how many arrived believing their body was somehow broken, that they were doing everything "right" and still not getting the results their male partners seemed to get effortlessly. So let me say this clearly, because it changes everything: your body is not broken. It's just running on different software. Women's physiology differs from men's not slightly but significantly, in how we store fat, respond to training, recover, and handle a calorie deficit. And almost all the mainstream advice you've absorbed was built on research done mostly on men, then scaled down and handed to you as if that were good enough. It isn't.
This guide is the one I always wished I could just hand to new clients on day one. It covers what women genuinely need to know: how your hormones shape fat loss, how to work with your menstrual cycle instead of against it, what shifts during perimenopause and postpartum, and how to build an approach that cooperates with your biology rather than fighting it. This is your complete starting point.
How Women's Physiology Differs
Body Composition
Women naturally carry a higher percentage of body fat than men, typically 22-26% essential fat for women vs 13-17% for men. This is not excess fat; it's biologically required for hormonal function, reproductive health, and pregnancy. Attempting to reduce below essential fat levels disrupts hormones severely.
Healthy body fat ranges for women:
| Category | Body Fat Range |
|---|---|
| Essential fat only (athlete extreme) | 10-13% |
| Athletic | 14-20% |
| Fit / healthy | 21-24% |
| Average | 25-31% |
| Above average | 32%+ |
→ Read more: Body Fat Percentage Guide for Women
Hormonal Influence on Fat Storage
Oestrogen influences where fat is stored. Premenopausal women tend to store fat in the hips, thighs, and buttocks (gluteofemoral fat), a hormonally protective pattern. As oestrogen declines in perimenopause and menopause, fat storage shifts to the abdominal region (visceral fat), which carries greater health risk.
This is why fat loss strategies must account for hormonal status, not just calories and exercise.
Metabolic Rate
Women have a lower basal metabolic rate than men of comparable size, primarily because women have a higher proportion of body fat (which is less metabolically active than muscle) and less lean mass. Muscle building is therefore even more important for women's long-term metabolic health than it is for men's.
→ Use the BMR Calculator for your resting metabolic rate.
Macros for Women: What's Different
The standard macro recommendations are built around male physiology. Women benefit from specific adjustments:
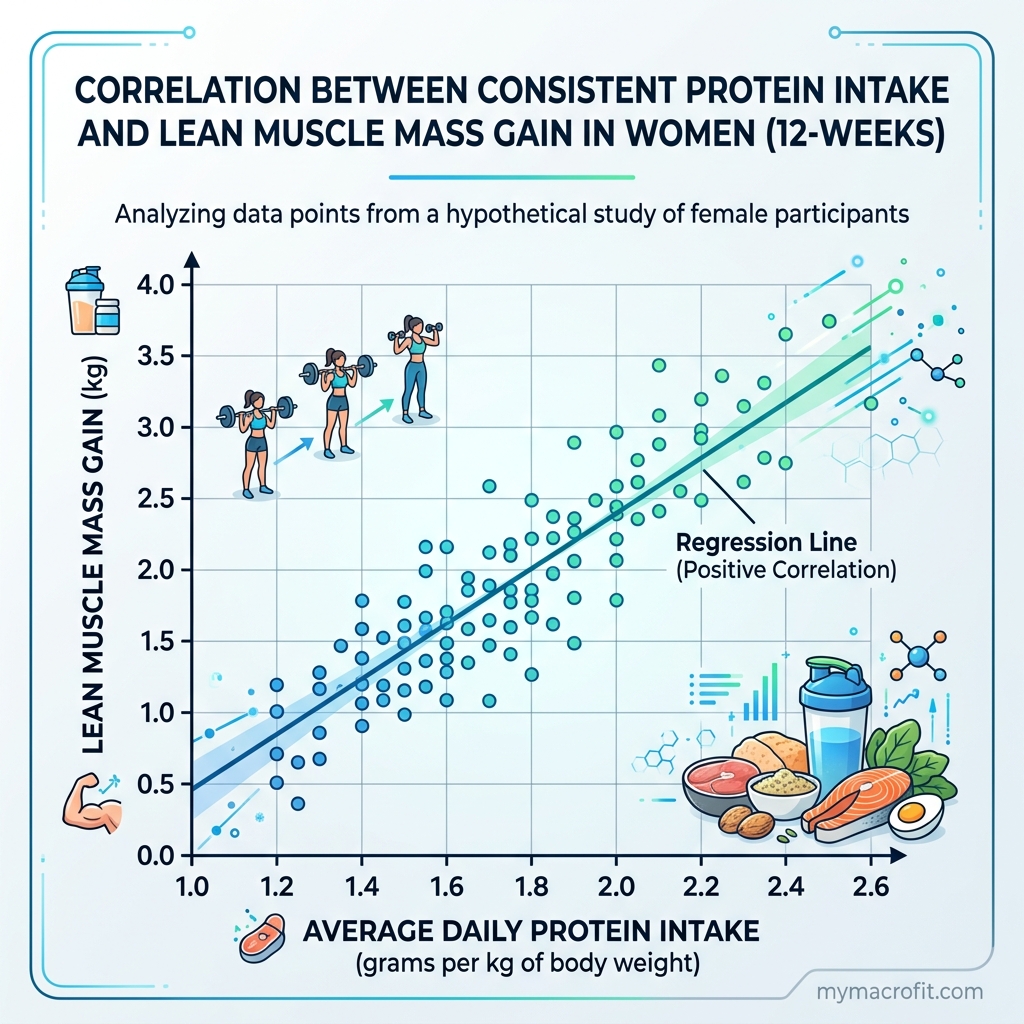
Higher Protein (More Important Than for Men)
Women are more susceptible to muscle loss during calorie restriction due to lower testosterone. Higher protein intake (1.8-2.2g/kg) is essential to preserve lean mass during a fat loss phase. The benefits of high protein, satiety, thermic effect, muscle preservation, are the same as for men, but the consequences of insufficient protein are more severe.
Practical protein targets by bodyweight:
| Bodyweight | Minimum protein (fat loss) | Optimal protein (fat loss) |
|---|---|---|
| 55kg | 99g/day | 121g/day |
| 65kg | 117g/day | 143g/day |
| 75kg | 135g/day | 165g/day |
| 85kg | 153g/day | 187g/day |
→ Read more: How Much Protein Do I Need? | Macro Calculator for Women
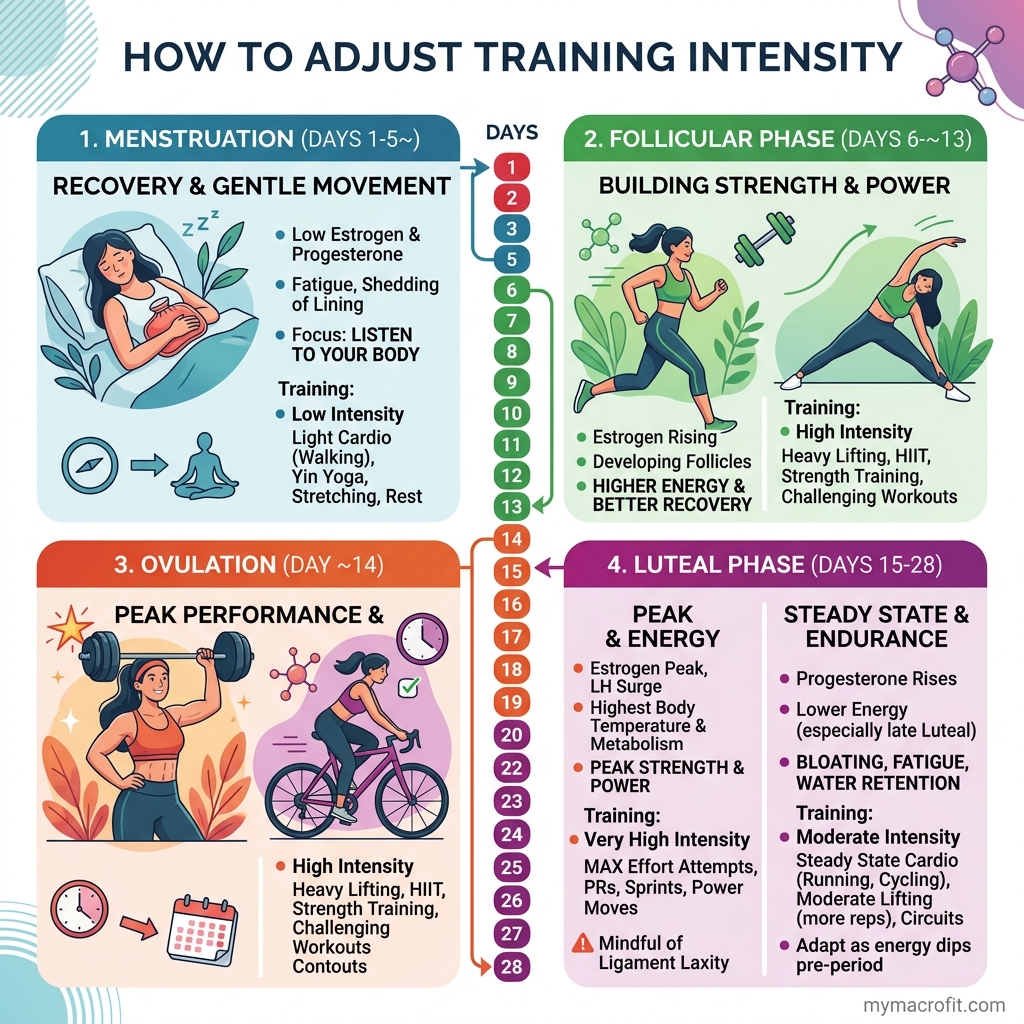
Carbohydrates and the Menstrual Cycle
Research suggests that insulin sensitivity fluctuates across the menstrual cycle. In the follicular phase (days 1-14), insulin sensitivity is generally higher, carbohydrates are better utilised. In the luteal phase (days 15-28), progesterone reduces insulin sensitivity, making high-carbohydrate meals more likely to cause energy crashes and cravings.
Practical adjustment:
- Follicular phase: maintain standard carb intake, higher-intensity training
- Luteal phase: slightly reduce carbs (−30-50g), increase fat to compensate, lower training intensity
This is the principle behind carb cycling, adjusting carb intake based on hormonal and energy status.
Fat and Hormonal Health
Women with very low fat intakes (below 20% of calories, or below 0.5g/kg) frequently experience hormonal disruption: irregular cycles, low oestrogen, reduced fertility, and poor mood. Dietary fat is the substrate for steroid hormone synthesis. Do not restrict fat below 0.7-1g/kg.

Strength Training for Women: The Case Is Overwhelming
The most important training decision a woman can make is to prioritise strength training. Yet most women default to cardio. Here's why this is the wrong approach:
What strength training does for women:
- Builds lean muscle, increasing resting metabolic rate
- Improves insulin sensitivity (protective against type 2 diabetes and PCOS)
- Increases bone mineral density (critical protection against osteoporosis post-menopause)
- Produces the "toned" appearance that cardio cannot, which is low body fat + visible muscle, not just low weight
- Improves functional strength and reduces injury risk
- Has strong evidence for reducing depression and anxiety
The "bulky" myth: Women do not produce enough testosterone to build large, bulky muscle without years of dedicated training and often pharmacological assistance. Strength training produces a lean, defined physique, not the bulky look most women fear.
Recommended starting programme:
- 3× per week full-body or upper/lower split
- Focus on compound movements: squat, hip hinge (deadlift/Romanian deadlift), push (press), pull (row/pulldown)
- Progressive overload: increase weight or reps each week
- Adequate protein (1.8-2.2g/kg) to support muscle repair
→ Read more: Build Muscle as a Woman | Strength Training for Weight Loss
Women-Specific Health Conditions
PCOS (Polycystic Ovary Syndrome)
PCOS affects approximately 1 in 10 women of reproductive age. Its central feature, insulin resistance, makes standard dietary advice insufficient. Women with PCOS need:
- Lower-GI carbohydrates (oats, legumes, sweet potato, berries over white rice, bread, juice)
- Higher protein intake (30%+ of calories) to improve insulin sensitivity
- Targeted supplements with evidence: inositol, berberine, magnesium, vitamin D, omega-3
- Resistance training, which is the most effective lifestyle intervention for insulin resistance
→ Read more: PCOS Diet and Macros: Complete Guide
Postpartum Nutrition and Weight Loss
The postpartum period is fundamentally different from any other fat loss context. Hormones, sleep deprivation, breastfeeding demands, and physical recovery all alter how the body responds to calorie restriction.
Key principles:
- No aggressive restriction before 8 weeks postpartum (6 weeks minimum for vaginal delivery)
- Breastfeeding women need 1,800-2,200 kcal minimum, do not create a significant deficit while exclusively breastfeeding
- Protein target: 1.5-2g/kg to support recovery and milk production
- Sleep is the highest-leverage variable, not diet, not exercise
→ Read more: Postpartum Weight Loss: A Realistic Timeline
Women Over 40 and Perimenopause
The hormonal transition from age 40 onwards, declining oestrogen and progesterone, directly affects body composition, fat distribution, and metabolic rate. Women often find that strategies that worked in their 30s become less effective.
What changes and what works:
- Fat redistributes to the abdomen, visceral fat increases even without weight gain; strength training is the most effective intervention
- Muscle mass declines more rapidly, protein needs increase; resistance training becomes non-negotiable
- Sleep worsens, night sweats, insomnia; prioritising sleep hygiene has metabolic benefits
- Cortisol sensitivity increases, stress management and adequate recovery become more important
→ Read more: How to Lose Belly Fat for Women Over 40
Intermittent Fasting for Women
Intermittent fasting (IF) compresses eating into a window (commonly 8 hours) and fasts for the remainder. It can be an effective tool for reducing total calorie intake for some women, but it requires more caution than for men.
Potential concerns for women:
- Extended fasting can disrupt the hypothalamic-pituitary-ovarian (HPO) axis in some women, particularly those who are lean or already in a calorie deficit
- Hormonal symptoms (irregular cycles, sleep disruption, mood changes) should prompt a reduction in fasting duration
- Not appropriate during pregnancy or postpartum breastfeeding
Modifications for women:
- Start with a 14:10 window rather than 16:8
- Place the eating window to include breakfast if morning hunger is significant
- Do not combine aggressive fasting with aggressive calorie restriction
→ Read more: Intermittent Fasting for Women: What You Need to Know
Building a Sustainable Approach
The research on long-term dietary adherence is unambiguous: the diet you stick to is more effective than the diet that's theoretically optimal. A 1,200 kcal plan with no flexibility has a six-month adherence rate close to zero for most women. A 1,600 kcal plan with room for meals out, social occasions, and preferences has adherence rates far higher.
Principles for sustainability:
-
Flexible dieting, not rigid rules, aim for 80% nutritious whole food, 20% flexible. Track the macros, not the food morality.
-
Protein first at every meal, this single habit makes everything else easier.
-
Plan for real life, restaurants, travel, social meals are not failures. They're life. Plan around them.
-
Progress over perfection, a week of poor tracking followed by a return to consistency is infinitely better than giving up entirely.
-
Train for performance, not punishment, strength training to get stronger, not to burn calories as penance.
-
Sleep as a non-negotiable, seven hours minimum. No training programme compensates for chronic sleep restriction.
Practical Starting Plan
Here's a simplified framework to start with:
Step 1: Calculate your calorie target → TDEE Calculator → set a 300-400 kcal deficit
Step 2: Set macros → Macro Calculator → prioritise protein at 1.8-2g/kg
Step 3: Structure meals → 3-4 meals per day, 30-40g protein each, vegetables at every meal, complex carbs, healthy fats
Step 4: Train → Strength training 3× per week, walking daily, cardio optional
Step 5: Adjust → Weigh weekly, assess monthly, adjust calories if progress stalls
Tools in This Guide
- Macro Calculator, personalised macro targets
- TDEE Calculator, daily calorie burn
- Protein Calculator, protein target by goal
- BMR Calculator, resting metabolic rate
- Body Fat Percentage Calculator, body composition tracking
All Articles in This Guide
Save & share on Pinterest
Click any card to pin it — or share with someone who needs it.
The Complete Women's Fitness Guide: Nutrition, Training, and Hormones
A comprehensive fitness and nutrition guide for women, covering macros, hormonal fat loss, PCOS, pos…
A comprehensive fitness and nutrition guide for women, covering macros, hormonal…
Read the full guide: The Complete Women's Fitness Guide: Nutrition, Training, and Hormones
Free fitness tools
The Complete Women's Fitness Guide: Nutrition, Training, and Hormones — use our free calculators for…
Pinterest opens in a new tab. You can edit the description before saving.
Frequently Asked Questions
Are nutrition guidelines different for women than men?+
Why is it harder for women to lose weight than men?+
What is the best exercise for women who want to lose fat and tone up?+
Should women eat differently at different points in their cycle?+
About the Author

I'm a kinesiologist and personal trainer. I've spent eight years helping women lose fat and get stronger without handing their whole life over to a diet.
View full profile →

